Modinomics = Corporatonomics
Part IV: Modi’s Budgets and the Social Sectors: Health
In the previous issues of Janata, we have analysed Modinomics and shown that the Modi Government, if it wants, can raise enough resources to increase its expenditures on the social sectors. Instead, it is giving away huge subsidies to the tune of several lakh crore rupees to the corporate houses. In this article, we specifically discuss Modi’s budget allocations for health.
State of India’s Health System
India’s health system is in “crisis”. India is the disease capital of the world:
- More than 2 lakh people in the country die of malaria every year, while TB kills 3 lakh;[i]
- According to the World Health Organisation (WHO), India accounts for nearly one-fourth of the deaths in the world due to diarrhoea, more than one-third of the deaths due to leprosy and more than half of the deaths due to Japanese encephalitis;[ii]
- India’s under-five child mortality rate is the highest in the world, with 12 lakh such deaths in 2015; a majority of these deaths are preventable;[iii]
- India is also in the grip of an epidemic of non-communicable diseases (long-term diseases such as diabetes, cardiovascular diseases [such as hypertension, heart attacks and stroke), chronic respiratory diseases (such as asthma) and cancers], which account for more than 60% of the deaths in the country.[iv]
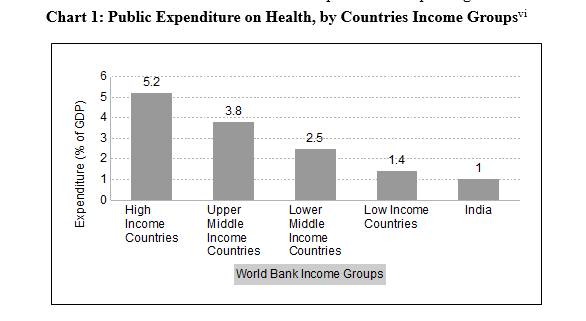
The reason for this ‘health emergency’ is the dismal state of India’s public health services. India spends barely 1.02% (in 2015–16) of its GDP on public health services, lower than even most low income countries, and far below the world average of 6% (see Chart 1). The WHO World Health Statistics 2015 ranked India at 187 out of 194 countries in public health spending.[v]
The difference between the health expenditure of developed countries and India becomes even starker when we compare the per capita GDP expenditure on health. The public health expenditure in the developed countries is as high as $3000–5000 per capita; it comes down sharply for developing countries like Thailand ($166 per capita), Sri Lanka ($63) and Indonesia ($38), but is only $16 per capital for India.[VII] This is equivalent to Rs 1,100 per person per year, less than the cost of consultation in one of the country’s top private hospitals. It works out to Rs 93 per month, or Rs 3 per day.
Consequently, the public health system in India is in bad shape. Around 33% of the population lives in urban areas. Since the focus of public health has been on rural areas since independence, primary urban health infrastructure remains grossly neglected. On the other hand, secondary and tertiary health care facilities are well developed in urban areas, and more than 60% of the government hospital beds in the country are located there (4.31 lakh out of 7.11 lakh, according to National Health Profile, 2018).
The rural health care infrastructure in India is a three-tier system—a sub‐centre, a Primary Health Centre (PHC) and a Community Health Centre (CHC). The sub-centre is the first contact point between the primary health care system and the community, caters to a population of between 3000–5000 people, is required to be staffed by at least one auxiliary nurse midwife (ANM)/female health worker and one male health worker, and provides services related to maternal and child health, family welfare, nutrition, etc. The PHC is the first base for doctors, and is the referral unit for around 6 sub-centres, and thus caters to a population of around 30,000. Therefore, it must have one medical officer, supported by paramedical and other staff, including one female and one male health assistant. The PHCs are supposed to screen and feed the more serious medical cases to CHCs (4 PHCs to 1 CHC), which are supposed to be staffed by at least four medical specialists, that is, surgeon, physician, gynecologist/obstetrician and pediatrician, along with supporting staff.
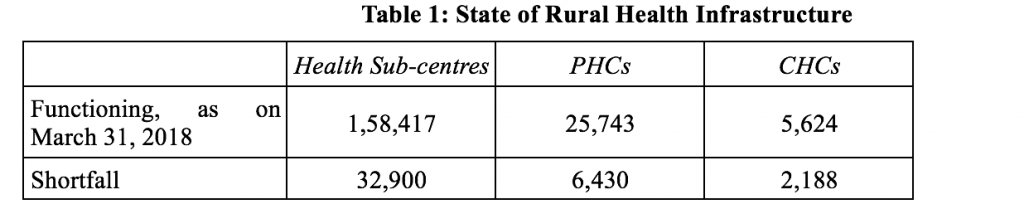
Even by standards set by the government, there is a 18% shortfall in the number of sub-centres, 22% in PHCs and 30% in CHCs in rural areas, as on March 31, 2018, according to Rural Health Statistics (RHS) Bulletin, 2017–18 (see Table 1).[viii]
Worse, of these currently functioning health centres, only 7% sub-centres, 12% PHCs and 13% CHCs are functioning as per Indian Public Health Standards (IPHS). The condition of the sub-centres is so bad that 16% do not have regular water supply, while 24.7% do not have electricity.[ix]
These health units are also severely deficient in hospital staff:
- Of the 1.58 lakh sub-centres functioning: 7,194 do not have ANMs, and 1,04,318 (66%) do not have male health workers, while 5,089 do not have both.
- Of the 25,743 PHCs functioning: 10,557 (41%) do not have female health assistants and 16,981 (66%) do not have male health assistants, while 3,673 do not even have a doctor.
- The 5,624 functioning CHCs suffer from a whopping 82% shortage of specialists (they have only 4,074 specialists out of the required 22,496). This huge shortfall makes redundant the rural health infrastructure. For instance, with no surgeons to man them, the 4,696 CHCs with functional operating theatres can only exist as empty structures.[x]
Including both rural and urban areas, the population–doctor (allopathic doctors only) ratio in India in 2017 was 11,082:1 in government hospitals, 25 times higher than the WHO recommendation of 25 professionals per 10,000 population. Likewise, the average population to government hospital ratio in the country was 55,951, which is also very high.[xi]
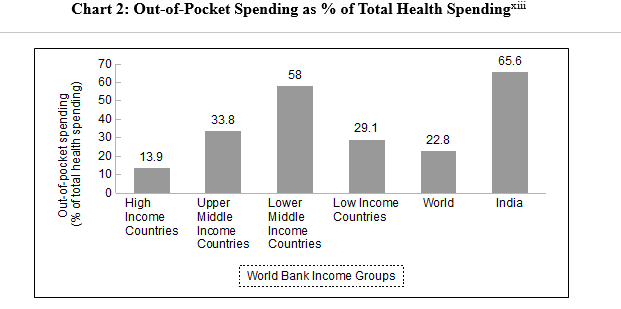
This dismal state of public health care has forced citizens to depend upon the private sector for treatment. Of the total health spending in the country, public health spending accounts for only 31.3%, households undertake the rest—at 65.6%, private expenditure on health care by Indians was the sixth highest in the world (among 184 nations surveyed), with the world average being 22.8% (see Chart 2). [This does not include health expenditure financed by private insurance; including this, private health spending by Indians increases to 68% of total health spending.][xii]
Because of lack of affordable medical services and high cost of private health care, an analysis based on data from NSSO 2014 showed that 3.6 crore households, or around 14% of total households in the country, incurred health expenses that exceeded the annual per capita consumption of those households. These figures underestimate the extent of health shock faced by the people of the country, as many people are simply too poor to go for any treatment even when a member faces a life-threatening disease. How many? This is difficult to say, but some clues can be had from NSSO data. The data says that while among the richest 5% people in the country, 98% received some kind of treatment before death, for the bottom 25%, a staggering 39% do not receive any medical attention before death. Maybe many of these poor people could have been saved had good quality and affordable health care been available in the country for all.[xiii]
Another study based on analysis of NSSO survey data of 2004 and 2014 estimates that more than five crore people were pushed into poverty over the decade 2004–14 due to out-of-pocket health spending.[xiv]
Modi–Jaitley Total Allocation for Health Care
The BJP came to power in 2014 promising to increase public health spending. Its manifesto stated that if it was voted to power, it would ensure that the orientation of the health care system would be to provide “Health Assurance to all Indians” and “reduce the out-of-pocket spending on health care”. Soon after assuming power, it released the draft National Health Policy (draft NHP 2015) that promised to increase the public health expenditure of the country to 2.5% of GDP, of which 40%, that is 1% of GDP, would be borne by the Centre. It promised to achieve these spending targets by 2020. Considering the dismal state of public health care in the country, this is obviously a very inadequate level of public health spending.[xv] The government took more than 2 years to finalise this report, and the final National Health Policy document was released only in 2017. It kept the spending target the same as that in the draft NHP 2015, but advanced the date for the target to be achieved to 2022.[xvi] As we have mentioned above, this target is less than half the global average public expenditure on health.
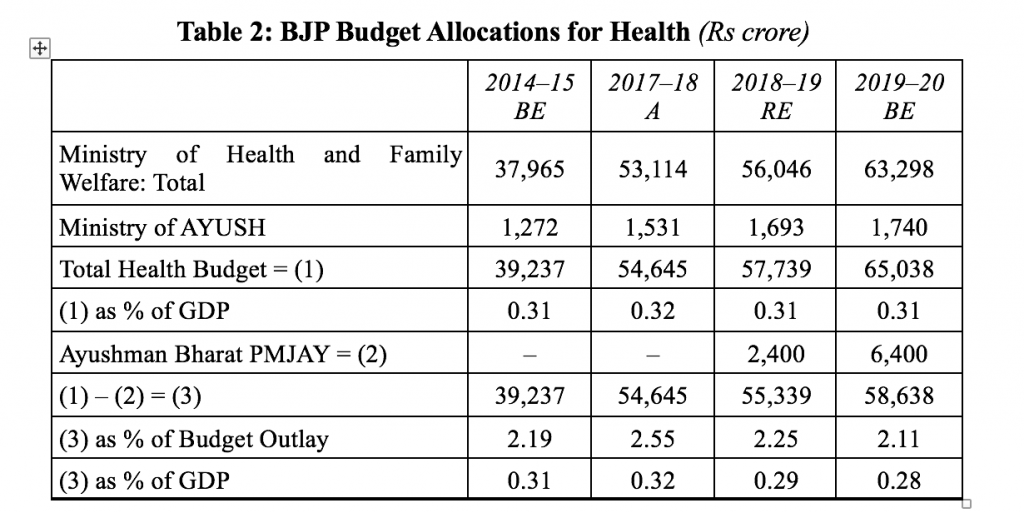
Be that as it may, since then, three budgets have gone by. The total expenditure on health care as a percentage of GDP has seen no increase during Modi’s five years and in 2018–19 BE was at the same level as in 2014–15 BE (at 0.31%); in 2019–20 BE too, it has remained at that level. Minus the allocation for the Ayushman Bharat health insurance scheme which does not go to improve the public health infrastructure in the country (discussed below), the health budget as a percentage of GDP has actually fallen, from 0.31% in 2014–15 BE and 0.32% in 2017–18 (A) to 0.29% in 2018–19 RE and 0.28% in 2019–20 BE—less than one-third of the target set in NHP 2017 (Table 2).
But then what about the Modi Government’s ambitious health programme, Ayushman Bharat or National Health Protection Mission, rolled out by the government last year? It hit the headlines in both the print and electronic media, and has been called a game-changer in terms of providing health care to the poor and needy.
Let us take a closer look at this much tom-tommed programme. It has two components: Ayushman Bharat Health and Wellness Centres (HWCs), and Pradhan Mantri Jan Arogya Yojana (PMJAY).
Health and Wellness Centres
In his 2018–19 budget speech, Jaitley announced a provision of Rs 1,200 crore for converting all the 1.5 lakh health sub-centres into Health and Wellness Centres (HWCs). He said that these would provide comprehensive health care, including for non-communicable diseases and maternal and child health services. He added that these centres will also provide free essential drugs and diagnostic services. The allocation for these HWCs is probably under the sub-head ‘Health Systems Strengthening’ within the head ‘National Rural Health Mission’, for which the budget had been increased by Rs 1,357 crore in the 2018–19 BE (over 2017–18 RE). The revised estimates show that the government spent Rs 1,000 crore on this. This works to an investment of Rs 63,000 for upgrading each health sub-centre.
Considering the terrible state of our rural health services, it is obvious that this allocation is simply too inadequate. The Rural Health Statistics 2017–18 point out that of the 1.58 lakh health sub-centres functioning, 16% do not have regular water supply and 24.7% do not have electricity; 7,194 health sub-centres do not have a female health worker, 1.04,318 do not have a male health worker, and 5,089 do not have both. For a sub-centre to become a Health and Wellness Centre, at the least, these basic facilities and human resources need to be provided. It is hard to understand how this can be done with the meagre funds allocated. The number of health sub-centres functioning is also less than required—the RHS points out that there is a shortage of 32,900 health sub-centres. Clearly, the finance minister has no intention of opening up new health centres to make up for this shortfall.
Further, what is the point in only improving the health sub-centres, if the referral centres for these basic health units, which are supposed to provide medical care by a qualified doctor, are not in good condition. As we have mentioned above, the conditions in the PHCs and CHCs are simply abysmal. More than 50% of the PHCs do not have health assistants, 3,673 do not have a doctor, and the CHCs suffer from 82% shortage of specialist doctors! But the finance minister has increased the allocation for Health System Strengthening by only 10.66% over the last two years, barely enough to beat inflation (Table 3).
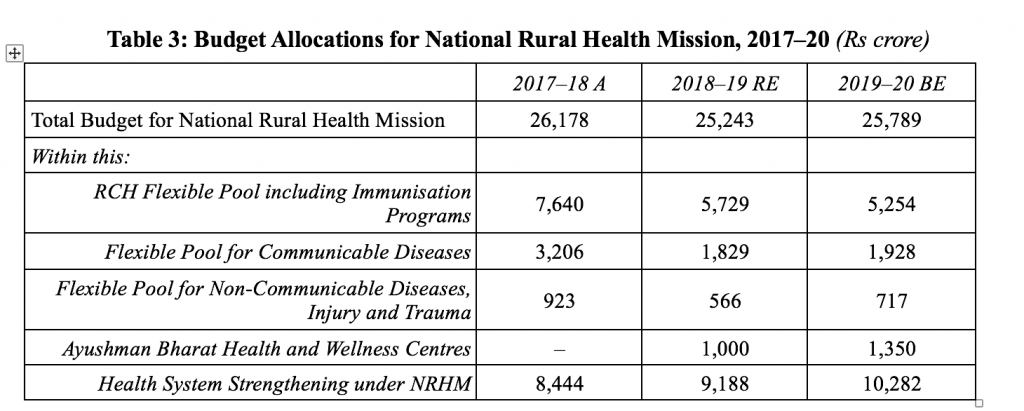
Actually, a closer look at the budget allocations reveal that like his several other announcements, this announcement of the finance minister regarding HWCs is also only a ‘jumla’. That he is absolutely non-serious about the improvement of rural health services becomes clear from the fact that the total budget for the National Rural Health Mission has actually decreased over the last two years even in nominal terms, which works out to an effective cut of 16% in real terms (see Table 3). The finance minister has succeeded in cutting total allocation for rural health services, while allocating money for HWCs, by slashing the budget allocation for other important rural health care programmes, such as ‘Flexible pool for non-communicable diseases (NCDs), injury and trauma’ which are the largest cause of death in the country,[i] and the important program for maternal and child care—‘RCH flexible pool including routine immunisation program and pulse polio immunisation program’ (see Table 3).
Urban Health Mission
The NRHM’s urban counterpart is the National Urban Health Mission (NUHM). The Union Cabinet had estimated the share of Central funding for this scheme to be around Rs 3,400 crore per annum way back in 2013 when it had given approval to this scheme aimed at addressing health care challenges in towns and cities with focus on the urban poor.[ii] However, the allocation for this has remained at much below this during the Modi regime: it was Rs 950 crore in the 2016–17 BE, but actual expenditure was only half of that, Rs 491 crore; allocation for it fell in subsequent years, and then rose back to Rs 950 crore in the 2019–20 BE. Clearly, the Modi Government is not serious about this scheme too.
While the Modi Government has reduced the budgets for the important rural and urban health missions, the budget allocation for the deceptively named Pradhan Mantri Swasthya Suraksha Yojana (PMSSY)—which is actually a scheme for building AIIMS-like institutes and upgrading government medical colleges—has been significantly increased in successive budgets. The allocation for this has gone up from Rs 2,450 crore in 2016–17 BE to Rs 3,875 crore in the 2018–19 RE to Rs 4,000 crore in 2019–20.
When we examine this increase in the backdrop of the reduction in the budgets for rural and urban health missions, it becomes clear that this is in tune with the overall approach of the Modi Government—build a few high quality facilities, amidst a huge expanse of neglect and ruin. This is what is happening in every sector—build a few airports, while neglecting basic transport infrastructure like the public bus transport system; build a few IITs, while neglecting school and college education, and so on. This does not mean that airports and IITs are not needed, but if funds are limited, priority should be given to improving primary transport and education facilities. Similarly, it is not that new high quality public tertiary hospitals are not needed—the problem is that this is being done while the primary health care sector is being neglected. If primary level health services are good—that is, if the PHCs and CHCs are running well—most illnesses can be taken care of at this level itself, and this will not only improve the efficiency and reduce the cost of delivery of public health services, it will also improve the overall health status of the people. Therefore, priority should be given to improving primary health care; but as we have discussed above, this has been neglected in the successive Jaitley budgets.
Ayushman Bharat Health Insurance Scheme
The other component of the Ayushman Bharat scheme is the Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (PMJAY). Jaitley proclaimed it to be “the world’s largest government funded health care programme”. Under this scheme, the government promised to provide medical insurance cover of Rs 5 lakh per family to 10 crore poor families (roughly 50 crore people) in case of hospitalisation (that is, out-patient care is not covered).
It is proof of the vacuity of our media that this announcement was highlighted by every TV news channel and hit the headlines of nearly every newspaper the next day. It was actually the biggest hoax of the budget.
Last year, Jaitley spent Rs 2,400 crore on this scheme as given in the 2018–19 RE, and this year, he has hiked the allocation to Rs 6,400 crore.
Even assuming that the finance minister is serious about providing medical insurance to the poor for hospitalisation, this increased allocation is simply not enough to provide the required insurance cover to 10 crore households. Various estimates suggest that the scheme could end up costing the government anywhere between Rs 12,000 crore to Rs 50,000 crore; with Jaitley allocating much less than even the lower of this estimate, obviously the government has no intention of meeting its target of providing health insurance to 10 crore people.[iii]
Do the poor really benefit from such health insurance schemes like the PMJAY? Some idea of it can be had from data regarding how many have benefited from the previous insurance scheme for the poor, Rashtriya Swasthya Bima Yojana (RSBY), which provided an insurance cover of Rs 30,000 per year to every BPL household in case of hospitalisation. The government has not been very willing to release RSBY data, and so comprehensive evaluations have not been done. Independent evaluations of the RSBY based on NSS data for 2014 show that only 1.2% of the hospitalisation cases of the rural population and 6.2% of the urban population received even part reimbursement. Studies have also shown that private hospitals often force people to pay extra money even after receiving RSBY insurance funds.[iv] Therefore, it is too early to say as to what extent will this new avatar of RSBY—PMJAY—will benefit poor families with regards to their hospitalisation expenses.
But the most serious problem with PMJAY is that it is not a universal health care scheme even for the poor. It does not cover out-patient costs, and these constitute 63.5% of the health related out-of-pocket expenditure (that is, personal spending by people) in India (data for 2014).[v] As mentioned above, India’s health-related out-of-pocket expenditure, which pushes families into indebtedness and deeper poverty, is among the world’s highest.
PMJAY: Excuse for Privatisation of Health Care
PMJAY does not cover out-patient expenses of the poor. It only meets their hospitalisation expenses—and past experience with similar insurance schemes raises legitimate doubts as to what extent will the poor benefit from this scheme. But the sectors that are undoubtedly going to enormously benefit from PMJAY are private hospitals and private insurance companies. It wouldn’t be an exaggeration to say that the real purpose of the PMJAY is to benefit them. The chief of the Ayushman Bharat scheme tweeted some time ago that private hospitals should quickly get themselves empanelled with the scheme as, “We are offering you business of 50 crore people!”[vi]
The Modi Government is in fact using the PMJAY as an excuse to accelerate the privatisation of health care in the country. The government has already announced incentives for the private sector to set up hospitals in Tier 2 and Tier 3 cities. These incentives include allotting unencumbered land for such hospitals, providing viability gap funding (VGF)—a euphemism for providing them grant of up to 40% of the project cost—and speeding up clearances. In November 2018, the Centre sent a note to all states asking them to sanction loans at agricultural rates of interest and provide electricity at residential rates to these private hospitals.[vii]
The private hospital business is one of the most profitable in the country. Most of our readers will have at least a few stories about how their friends and relatives have been fleeced by private hospitals. And yet the government wants to incentivise the setting up of more private hospitals, and even provide them a grant (not a loan) of up to 40% of the cost of the project!
As if this was not enough, Niti Aayog and the health ministry have recommended to all states that they partially privatise their district hospitals, and transfer sections of these hospitals, including land and a certain number of hospital beds, to private players.[viii] The Niti Aayog guidelines for these ‘public-private-partnerships’ (PPPs) imply that the staff of these district hospitals would now be basically engaged in PPP implementation, referring patients to the private doctors and facilitating the reimbursement of expenditure of individuals incurred in PPP facilities.[ix]
Hospitalisation constitutes only a small part of the total health expenses of any individual, as not every disease needs hospitalisation. Even diseases like diabetes and respiratory problems and heart problems only require hospitalisation if the patient’s condition takes a turn for the worse. And since PMJAY covers only hospitalisation costs, this means that as the privatisation of government hospitals advances, out-patient costs are going to go up sharply, which the poor will not be able to afford—it is going to further worsen the health crisis gripping the country.
Additionally, many lower middle class and middle class families not covered by PMJAY also go to government hospitals as they cannot afford private medical care. Privatisation of government hospitals is going to mean that in case they fall seriously ill and need to be hospitalised, it would mean catastrophic medical expenses for them.
Under the guise of rolling out the world’s largest health care initiative, the anti-people Modi Government is actually seeking to destroy whatever that remains of India’s failing public health care system and privatise it. It is going to have terrible consequences for the people.
Can’t Jaitley Increase the Health Budget?
The only way in which reliable and good quality health care can be provided to ordinary people is by strengthening public health care facilities—and thereby provide them both out-patient and hospitalisation care free or at affordable rates. That is what governments have done around the world. To do that in India, the Indian government needs to increase its health care budget.
The NHP promises to increase Central government health spending to 1% of GDP, and total Central and State government spending on health to 2.5% of GDP. That is a very low target, it should be increased to at least 3% of GDP, and more subsequently. Presently, the expenditure on health is 1% of GDP; so that means the total initial increase in spending on health by the Centre + States should be at least 2% of GDP or Rs 4.2 lakh crore. As we have shown in our previous articles, it is not that the government cannot raise the required funds to make this allocation; it is a question of priorities—whether priority should be given to profiteering of corporations, or providing essential health and education facilities to the people.
The media headlines have got it all wrong. The Modi Government’s health budget is not about the world’s largest health protection plan. It is about a country which has the highest number of deaths in the world due to disease, a country with the highest number of child and maternal deaths in the world, criminally neglecting this health ‘crisis’ and spending less than almost all other countries in the world on improving public health facilities—while at the same time giving lakhs of crores of rupees as subsidies to its uber rich.
References
[i] “Health Budget Focuses Only on Ayushman Bharat, Other Schemes Ignored”, February 2, 2019, https://www.livemint.com
[ii] “Urban Health Mission to Cover 7.75 Crore People”, May 2, 2013, http://www.thehindu.com.
[iii] Deepshikha Sikarwar, Vinay Pandey, “Modicare: Healthcare Scheme Could Cost Exchequer Rs 10,000 Crore a Year”, February 3, 2018, https://economictimes.indiatimes.com; Anoo Bhuyan, “Explained: Why Healthcare Reforms Should Be an Election Issue in 2019”, February 26, 2019, https://thewire.in.
[iv] Anoo Bhuyan, “Budget 2018: Jaitley’s ‘World’s Largest Health Programme’ Rejigs Flailing Old Ones”, February 1, 2018, https://thewire.in; Dipa Sinha, “Neglecting Health Expenditure in Favour of the Chimera of Insurance”, February 29, 2016, https://thewire.in.
[v] Prachi Salve, Swagata Yadavar, “Why Rashtriya Swasthya Bima Yojana Has Failed India’s Poor”, October 19, 2017, http://smartinvestor.business-standard.com.
[vi] “Budget 2019: Ayushman Bharat Gets Rs 6,400 Crore, But to Benefit Private Sector”, February 1, 2019, https://thewire.in.
[vii] “In the Wake of Ayushman Bharat Come Sops for Private Hospitals”, January 9, 2019, https://thewire.in; “Only a Strong Public Health Sector Can Ensure Fair Prices and Quality Care at Private Hospitals”, March 28, 2019, https://scroll.in.
[viii] Ibid.
[ix] Shailender Kumar Hooda, “With Inadequate Health Infrastructure, Can Ayushman Bharat Really Work?”, November 26, 2018, https://thewire.in.
Read more